

Chewing The Fat Factsheet
How a plant-based diet provides all the essential fats you need – and why animal fats are particularly detrimental to health
By: Amanda Woodvine, BSc Nutrition Viva!Health (formerly VVF) Senior Nutritionist, with additional research from Dr Justine Butler, Viva!Health Senior Research & Writer
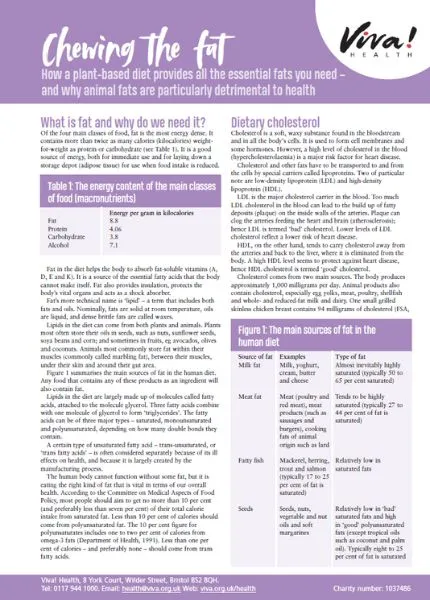
What is Fat and Why Do We Need It? Of the four main classes of food, fat is the most energy dense. It contains more than twice as many calories (kilocalories) weightfor-weight as protein or carbohydrate (see Table 1). It is a good source of energy, both for immediate use and for laying down a storage depot (adipose tissue) for use when food intake is reduced.
What is Fat and Why Do We Need It?
Of the four main classes of food, fat is the most energy dense. It contains more than twice as many calories (kilocalories) weight for-weight as protein or carbohydrate (see Table 1). It is a good source of energy, both for immediate use and for laying down a storage depot (adipose tissue) for use when food intake is reduced.
Fat in the diet helps the body to absorb fat-soluble vitamins (A, D, E and K). It is a source of the essential fatty acids that the body cannot make itself. Fat also provides insulation, protects the body’s vital organs and acts as a shock absorber.
Fat’s more technical name is ‘lipid’ – a term that includes both fats and oils. Nominally, fats are solid at room temperature, oils are liquid, and dense brittle fats are called waxes.
Lipids in the diet can come from both plants and animals. Plants most often store their oils in seeds, such as nuts, sunflower seeds, soya beans and corn; and sometimes in fruits, eg avocados, olives and coconuts. Animals most commonly store fat within their muscles (commonly called marbling fat), between their muscles, under their skin and around their gut area.
Lipids in the diet are largely made up of molecules called fatty acids, attached to the molecule glycerol. Three fatty acids combine with one molecule of glycerol to form ‘triglycerides’. The fatty acids can be of three major types – saturated, monounsaturated and polyunsaturated, depending on how many double bonds they contain.
A certain type of unsaturated fatty acid – trans-unsaturated, or ‘trans fatty acids’ – is often considered separately because of its ill effects on health, and because it is largely created by the manufacturing process.
The human body cannot function without some fat, but it is eating the right kind of fat that is vital in terms of our overall health. According to the Committee on Medical Aspects of Food Policy, most people should aim to get no more than 10 per cent (and preferably less than seven per cent) of their total calorie intake from saturated fat. Less than 10 per cent of calories should come from polyunsaturated fat. The 10 per cent figure for polyunsaturates includes one to two per cent of calories from omega-3 fats (Department of Health, 1991). Less than one per cent of calories – and preferably none – should come from trans fatty acids.
Dietary Cholesterol
Cholesterol is a soft, waxy substance found in the bloodstream and in all the body’s cells. It is used to form cell membranes and some hormones. However, a high level of cholesterol in the blood (hypercholesterolaemia) is a major risk factor for heart disease.
Cholesterol and other fats have to be transported to and from the cells by special carriers called lipoproteins. Two of particular note are low-density lipoprotein (LDL) and high-density lipoprotein (HDL).
LDL is the major cholesterol carrier in the blood. Too much LDL cholesterol in the blood can lead to the build up of fatty deposits (plaques) on the inside walls of the arteries. Plaques can clog the arteries feeding the heart and brain (atherosclerosis); hence LDL is termed ‘bad’ cholesterol. Lower levels of LDL cholesterol reflect a lower risk of heart disease.
HDL, on the other hand, tends to carry cholesterol away from the arteries and back to the liver, where it is eliminated from the body. A high HDL level seems to protect against heart disease, hence HDL cholesterol is termed ‘good’ cholesterol.
Cholesterol comes from two main sources. The body produces approximately 1,000 milligrams per day. Animal products also contain cholesterol, especially egg yolks, meat, poultry, shellfish and whole- and reduced-fat milk and dairy. One small grilled skinless chicken breast contains 94 milligrams of cholesterol (FSA, 2002), whereas foods from all plants (every type of fruit and vegetable, pulses, (peas, beans and lentils) wholegrains, nuts and seeds) are cholesterol-free.
Humans have no need for dietary cholesterol as the body can manufacture all that it requires. The American Heart Association recommends that people limit their average daily cholesterol intake to no more than 300 milligrams (AHA, 2008).
High intakes of dietary cholesterol increase harmful LDL cholesterol (Grundy and Denke, 1990) which can increase the risk of heart disease. If you are genetically prone to hypercholesterolaemia then it is especially important to restrict dietary cholesterol, which is found in all animal products. Highquality proteins from vegetable sources such as pulses are good substitutes for animal sources of protein. For more information, see the guide, Have a Heart.
Saturated Fatty Acids
We have no nutritional need for saturated and monounsaturated fats as the body can make them. Diets high in saturated fat and calories raise blood cholesterol levels and contribute to cardiovascular disease, diabetes and some cancers. Saturated fat has 10 times the cholesterol-raising power of dietary cholesterol (Enas et al., 2003). Furthermore, foods high in saturated fat generally contain substantial amounts of dietary cholesterol. Reducing total and saturated fat intakes could also lower the risk of breast cancer (see the report, One in Nine).
Not all saturated fatty acids have the same effects. Those which raise cholesterol the most are lauric acid, myristic acid, and palmitic acid, which are found in meat, dairy products, eggs and tropical oils. These three fatty acids account for 60 to 70 per cent of the saturated fat in Western diets.
Myristic acid is the most powerful cholesterol-raising saturated fatty acid (Kris-Etherton et al., 1997). The major dietary sources of myristic acid are butter, cream, whole milk and tropical oils. Milk fat (from dairy cows) contains eight to 14 per cent myristic acid. Coconut and palm oils contain up to 18 per cent (German et al., 2004).
Palmitic acid is the most common fatty acid in the human diet. It is the main saturated fatty acid in animal fats (including red meats, poultry and eggs) and in palm oil.
Lauric acid is the least harmful of these three saturated fats, with around one-third less cholesterol-raising power than palmitic acid. It is the main saturated fatty acid in coconut and palm kernel oils (they contain around 48 per cent) (Grundy, 1986; Renaud and Delorgel, 1989; Katan et al., 1995).
As tropical oils such as coconut and palm do not feature heavily in our typical national diet, they do not contribute significantly to average national saturated fat intake (FSA/Department of Health, 2003). However, coconut is the main source of energy for certain Polynesian populations. The habitual diets of the toll dwellers from both Pukapuka and Tokelau are high in saturated fat (primarily from coconut) but low in dietary cholesterol (found only in animal products) and sucrose (sugar).
Tokelauans take in many more calories from coconut than the Pukapukans (63 per cent compared with 34 per cent) and therefore have higher intakes of saturated fat. As might be expected, Tokelauans have higher blood cholesterol levels. However, cardiovascular disease – the build up of lipids and other cells on the artery wall – is still surprisingly rare in both populations (Prior et al., 1981).
This apparent paradox might be explained by coconut’s fibre content. Coconut is a good source of soluble and insoluble dietary fibre which have cholesterol-lowering powers. Coconut flakes (rather than coconut oil) have been found to lower harmful (LDL) cholesterol levels (Trinidad et al., 2004). Of course, processing coconut in order to produce coconut oil does strip away the protective fibre.
Conversely, the leading sources of harmful saturated fats in the British national diet – namely dairy products and meat – contain no protective, cholesterol-lowering fibre (FSA, 2002; FSA/Department of Health, 2003). As perhaps would be expected, cardiovascular disease is a common finding in people who consume the modern Western diet. For more information, see the fact sheet, Plant-based Diets and Cardiovascular Disease.
Trans-unsaturated Fatty Acids
Trans fatty acids have also been shown to increase the risk of heart disease by raising harmful (LDL) cholesterol levels and lowering protective (HDL) cholesterol levels. Their combined effect on LDL and HDL cholesterol is twice that of saturated fatty acids (Mensink and Katan, 1990).
Gram for gram, trans fats are even more strongly linked to heart disease than saturated fats. A review of trans fats’ effects on health found them to be associated with a two-and-a-half to tenfold higher risk of heart disease than saturated fats (Stender and Dyerberg, 2004). No safe limits of trans fat consumption have been identified (Murray, 2005).
Trans fatty acids are often found in processed foods. An industrial process known as hydrogenation is often used to convert liquid vegetable oils to solid or semi-solid fats, such as those present in margarine. The final product of this process is called hydrogenated vegetable oil, or hydrogenated fat. It is used in some biscuits, cakes, pastry, margarine and many processed foods. Foods that contain hydrogenated vegetable oil (which is always declared in the ingredients list) are likely to contain trans fats. By avoiding products containing hydrogenated fats or oils the trans fat content of a plant-based diet can be kept desirably low.
Low levels of trans fatty acids are also found naturally in dairy products, lamb and beef fat. This is because small amounts of trans fats are produced in the gastrointestinal tract of ruminant animals (Murray, 2005).
Essential Fatty Acids
The fats which are essential to the diet are linoleic acid (from the omega-6 family of fatty acids) and alpha-linolenic acid (omega-3 family). Dietary sources of these essential fatty acids, or EFAs, are listed in Table 4. Seed oils such as flax (linseed), rapeseed (canola) and walnut oil are rich sources of EFAs as are seeds and nuts themselves (Buttriss, 1999). Green leafy vegetables are also a source (Pereira et al., 2001).
Polyunsaturated fatty acids have many important functions in the body. They have a structural function in cell membranes; can aid the retina and other organs, including the brain and skin; are involved in regulating the transport, breakdown and excretion of cholesterol; and are precursors of prostaglandins, thromboxane and leukotrienes, which regulate many body processes including inflammation and blood clotting.
There are at least three important fatty acids in the omega-3 family: ALA, EPA and DHA. ALA can be obtained from flaxseed (linseed) oil, walnuts, rapeseed, soya beans and green leafy vegetables (although the latter do not contain much as they are generally very low in fat) (see Table 4). EPA and DHA – which are required for brain function – can only be obtained from marine sources, namely oily fish and some species of algae. However, ALA can be converted into EPA and DHA in the body.
Likewise, LA, found in sunflower, corn, walnut and soya oils, can be converted into other important polyunsaturated fatty acids in the omega-6 family, such as arachidonic acid.
Omega-3: Fish versus Flax
A major review published in the British Medical Journal (Hooper et al., 2006) supports the view that pollutants in fish, such as mercury, dioxins and polychlorinated biphenyls, may cancel out the beneficial effects of the ‘good’ omega-3 fats they contain.
The good news is there are perfectly safe plant sources of omega-3 that can benefit health. Many studies, including a joint report by the World Health Organisation and Food and Agriculture Organisation show that ALA has a protective effect against heart disease. This benefits the environment as well; flax is a sustainable crop whereas fish are not. (For more information, see the VVF’s Fishing for Facts fact sheet.)
Recent studies suggest that the ratio of omega-6 to omega-3 fatty acids is more important than the amounts of individual fatty acids consumed. Recent changes in the diet, as we have moved away from whole foods towards refined foods rich in processed vegetable oils, have increased our intake of omega-6 fats. This has increased the ratio of omega-6 to omega-3 fats in the diet, which may have a detrimental effect on the rate of conversion of ALA to EPA and DHA.
Most people eating a Western diet need to limit the amount of omega-6 essential fats in their diet and increase the amount of omega-3. This can be achieved by reducing the use of omega-6 rich sunflower, safflower and corn oils and increasing the use of omega-3 rich flaxseed and rapeseed oils.
Cutting down on dietary cholesterol (avoiding eggs, meat and dairy products), avoiding or cutting down on processed foods, and avoiding foods containing hydrogenated vegetable oils (listed on the packaging) will help your body make best use of the omega-3 from plant foods.
Also avoid or reduce fried foods, alcohol, caffeine, sugar, smoking and stress. Make sure that you get all the minerals you require including zinc – found in pulses, wholegrains (eg brown rice, wholemeal bread etc), nuts and seeds – and chromium, found in nuts, wholegrains and brewer’s yeast.
One teaspoon of flaxseed oil or one-and-a-half tablespoons of ground flaxseed should provide most people with sufficient omega-3 fats (see Table 5). These fats are easily damaged by light or heat so try and keep these foods refrigerated and use them cold, for example on cold vegetable/rice/pasta salads and so on.
Summary
- Reduce your intake of saturated fat, dietary cholesterol, and trans-unsaturated fatty acids
- Avoid products containing hydrogenated fats or oils (listed on the packaging)
- Avoid butter, cream, whole milk and tropical oils as they are especially rich in cholesterol-raising saturated fats
- If you are genetically prone to hypercholesterolaemia then it is particularly important for you to restrict dietary cholesterol, which is found in all animal products
- Improve the balance of omega-6 to omega-3 in your diet by reducing omega-6 oils (sunflower, corn oil) and increasing omega-3s (flax, rapeseed)
- Pollutants in fish may cancel out the beneficial effects of the ‘good’ omega-3 fats they contain
- ALA (from plant foods) can be converted into EPA and DHA, and has a protective effect against heart disease
- Cutting down on dietary cholesterol (eggs, meat and dairy products), processed foods, and hydrogenated vegetable oils will help your body to make best use of the omega-3 from plant foods
- Also avoid or reduce fried foods, alcohol, caffeine, sugar, smoking and stress
- Increase the consumption of foods rich in fibre, including wholegrains, fruit and vegetables
References
- AHA, 2008. Cholesterol AHA Scientific Position [online]. AHA. Available from: http://www.americanheart.org/presenter.jhtml?identifier=4488 [Accessed 17 January 2008].
- British Nutrition Foundation, 2000. BNF Nutrition Papers. n-3 Fatty Acids and Health [online]. BNF. Available from: http://www.nutrition.org.uk/home.asp?siteId=43§ionId=686&subSectionId=341&parentSection=303&which=6#1171 [Accessed 20 October 2008].
- Department of Health, 1991. Dietary Reference Values for Food Energy and Nutrients for the United Kingdom. Report of the Panel on Dietary Reference Values of the Committee on Medical Aspects of Food Policy. London: HMSO.
- Enas A., Senthilkumar A., Chennikkara H. and Bjurlin M.A., 2003. Prudent diet and preventive nutrition from pediatrics to geriatrics: current knowledge and practical recommendations. Indian Heart J. 55 (4), 310–338.
- Food Standards Agency, 2002. McCance and Widdowson’s The Composition of Foods, Sixth Summary Edition. Cambridge: Royal Society of Chemistry.
- Food Standards Agency/Department of Health, 2003. The National Diet & Nutrition Survey: Adults aged 19 to 64 years. London: TSO.
- German J.B. and Dillard C.J., 2004. Saturated fats: what dietary intake. Am J Clin Nutr. 80 (3), 550-9.
- Grundy S.M., 1986. Comparison of monounsaturated fatty acids and carbohydrates for lowering plasma cholesterol. N Engl J Med. 314 (12), 745–748.
- Grundy S.M. and Denke M.A, 1990. Dietary influences on serum lipids and lipoproteins. J Lipid Res. 31 (7), 1149-1172.
- Hooper L., Thompson R.L., Harrison R.A., Summerbell C.D., Ness A.R., Moore H.J., Worthington H.V., Durrington P.N., Higgins J.P., Capps N.E., Riemersma R.A., Ebrahim S.B. and Davey Smith G., 2006. Risks and benefits of omega 3 fats for mortality, cardiovascular disease, and cancer: systematic review. BMJ. 332 (7544), 752-60.
- Katan M.B., Zock P.L. and Mensink R.P., 1995. Dietary oils, serum lipoproteins, and coronary heart disease. Am J Clin Nutr. 61 (Suppl), 1368S–1373S.
- Kris-Etherton P.M. and Yu S, 1997. Individual fatty acid effects on plasma lipids and lipoproteins: human studies. Am J Clin Nutr. 65 (suppl), 1628S-44S.
- Mensink R.P.M. and Katan MB, 1990. Effect of dietary trans fatty acids on health. Ann Nutr Metab. 48 (2), 61-6.
- Murray S., 2005. Chewing the fat on trans fats. CMAJ. 173 (10), 1158-1159.
- Pereira C., Li D. and Sinclair A.J., 2001. The alpha-linolenic acid content of green vegetables commonly available in Australia. Int J Vitamin Nutr Res. 71 (4), 223-228.
- Prior I.A., Davidson F., Salmond C.E. and Czochanska Z., 1981. Cholesterol, coconuts, and diet on Polynesian atolls: a natural experiment: the Pukapuka and Tokelau Island studies. Am J Clin Nutr. 34 (8), 1552-61.
- Renaud S. and Delorgel M., 1989. Dietary lipids and their relation to ischemic heart disease from epidemiology to prevention. J Int Med. 225 (Suppl), 39–46.
- Stender S. and Dyenberg J., 2004. Influence of trans fatty acids on health. Ann Nutr Metab. 48 (2), 61-6.
- Trinidad T.P., Loyola A.S., Mallillin A.C., Valdez D.H., Askali F.C., Castillo J.C., Resaba R.L. and Masa D.B., 2004. The cholesterol-lowering effect of coconut flakes in humans with moderately raised serum cholesterol. J Med Food. 7 (2), 136-40.
This post has been categorised in: All Print Materials, Factsheets